
Please Support Talking-up Scotland at:
https://www.crowdfunder.co.uk/p/support-talking-up-scotland
Click on the above.
Or direct bank transfer at Sort Code 08-91-04 Account - 12266421 Name - JOHN ROBERTSON
From BBC England today, the above and:
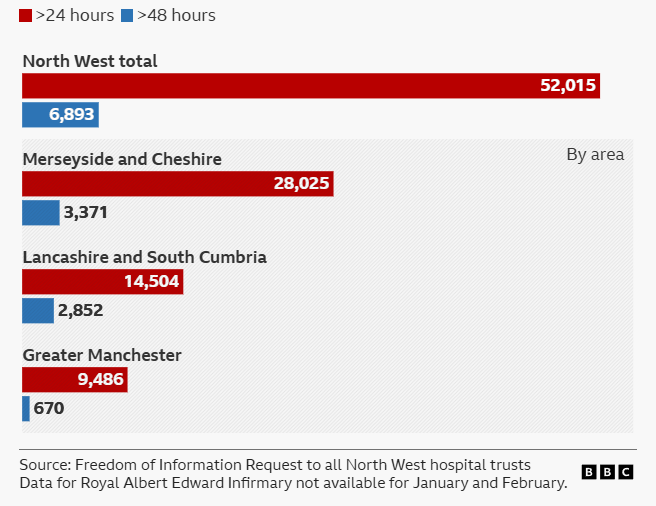
More than 52,000 patients waited longer than 24 hours to be admitted to hospitals across north-west England last year, a BBC investigation has revealed. Known as “corridor care”, patients are lining up on trolleys or sitting on chairs, stuck in A&E because there are no beds for them in the wards. The Royal College of Nursing has described the situation as a “national emergency” and called on the government to end the practice.
BBC England’s measure of the level of corridor care on objective waiting times statistics is correct.

The Herald above, in February 2026, based on unreliable statistical methods by the Daily Record (No surprise there) has misrepresented the level of ‘corridor care‘ in Scotland’s hospitals. BBC Scotland, then simply spread them, uncritically.
Explicit figures are not published anywhere but there’s a good proxy for corridor care and that’s 12 hour or longer waits in A&E. By definition if you’re waiting 12 hours after triage assessment and maybe some treatment before getting a bed, that is ‘corridor care.’ A fuller AI rationale for the use of 12 hour waits, based heavily on the views of the Royal College of Medicine, Age Concern and even NHS England itself, is below.
A&E demand varies from month to month and, of course peaks in the winter months, so comparing one month, December, over the last four years is revealing.

So, all A&E waits are lower than they were 4 years ago and lower than they were last year. The first media reports of ‘corridor care’ in Scotland were around July 2024. Given that A&E waits, especially 12 hour waits, are now significantly lower than in 2024, that suggest politics rather than facts.
Further, the discussion of methods below points to: In England, the key metric is 12 hours from decision to admit (most precise for corridor care). In Scotland (and sometimes advocated UK-wide), it’s often 12 hours from arrival, which includes initial assessment time and may overestimate pure corridor waits.
Sources:
Please Support Talking-up Scotland at:
https://www.crowdfunder.co.uk/p/support-talking-up-scotland
Click on the above.
Or direct bank transfer at Sort Code 08-91-04 Account - 12266421 Name - JOHN ROBERTSON
Methods:
Why 12-Hour or greater A&E Waits Are a Good Proxy for Corridor Care
Corridor care (also called trolley waits or care in temporary escalation spaces) occurs when emergency departments (EDs) are overcrowded due to a lack of inpatient beds, forcing patients who need admission to be treated in non-clinical areas like corridors, waiting rooms, or chairs. This is unsafe, undignified, and linked to patient harm.The most accurate proxy in NHS data—particularly in England—is the number of patients waiting more than 12 hours from the decision to admit (DTA) to actual admission (known as “12-hour trolley waits” or “12-hour DTA waits”). Here’s why this metric strongly indicates corridor care:
- Direct Link to Bed Availability Delays
Once a clinician decides a patient needs admission (DTA), the wait is almost entirely due to no available ward bed. Patients remain in the ED, often on trolleys in corridors or other overflow areas, receiving ongoing care there. Short DTA waits mean quick transfers to proper wards; prolonged waits (especially >12 hours) mean patients are stuck in unsuitable ED spaces. - Official and Expert Recognition
- NHS England and the Royal College of Emergency Medicine (RCEM) explicitly link these waits to corridor care. For example, NHS spokespeople have stated: “It is totally unacceptable that patients are waiting over 12 hours to be admitted to a hospital bed, and in some cases, this wait is occurring in corridors.”
- The Royal College of Nursing (RCN) describes 12-hour waits as “the clearest indicator of corridor care taking place,” since staff cannot move admitted patients to wards.
- Age UK and Liberal Democrat analyses equate 12-hour trolley waits directly with corridor care experiences.
- No Direct National Tracking of Corridor Care
The NHS does not routinely publish data on the exact number of patients treated in corridors (though some site-specific or survey data exists). In its absence, 12-hour DTA waits serve as the best available quantitative proxy, capturing the severity of exit block (delayed transfers out of ED). - Evidence of Harm and Scale
RCEM research shows long waits (8–12 hours and beyond) are associated with excess mortality (e.g., one additional death per 72 patients waiting 8–12 hours). These waits overwhelmingly occur in corridor-like settings during overcrowding.
Note on Variations in Measurement
- In England, the key metric is 12 hours from DTA (most precise for corridor care).
- In Scotland (and sometimes advocated UK-wide), it’s often 12 hours from arrival, which includes initial assessment time and may overestimate pure corridor waits.
Both are used as proxies, but DTA is more specific to the bed-delay phase where corridor care predominates.
In summary, 12-hour waits (especially DTA) reliably signal when ED overcrowding forces care into corridors, making them a vital—though imperfect—measure of this systemic issue. Experts like RCEM presidents call it a “national shame” and urge its elimination through better bed capacity and flow.
Please Support Talking-up Scotland at:
https://www.crowdfunder.co.uk/p/support-talking-up-scotland
Click on the above.
Or direct bank transfer at Sort Code 08-91-04 Account - 12266421 Name - JOHN ROBERTSON
Discover more from The 'Unstoppable' Talking-up Scotland
Subscribe to get the latest posts sent to your email.

The author of the BBC News website article on the damning statistics on ‘corridor care’ in NHS hospitals in NW England tells readers this: ‘The reasons for the current situation are complex and most are out of the control of the hospitals themselves.’
Out of hospitals’ control – Imagine someone from BBC Scotland writing this?
The article adds: ‘A major factor is the crisis in social care provision, which sees older, more frail patients trapped in hospital beds for days or even weeks because a suitable care package cannot be found.’ So what is happening to social care in the UK nowadays?
From November 21, 2025 in a press statement from Scottish Care: ‘Scottish Care Warns Immigration Proposals Threaten Scotland’s Care Sector.’
‘Scottish Care is deeply concerned by the Home Secretary’s proposals to extend the qualifying period for settlement for legal migrants, particularly the increase from five to fifteen years for those on health and social care visas. These changes will have a profoundly negative impact on the sustainability and quality of care and support services across Scotland.’
And notes: ‘Their impact especially in Scotland’s remote and rural communities is incalculable. They also send a damaging message that the invaluable contributions of migrant care workers are not fully recognised or valued. Scottish Care urges the UK Government to reconsider these proposals and to work with devolved administrations to ensure immigration policy supports, rather than hinders, the future of care in Scotland.’
Back to England, from a Royal College of Nursing (RCN) press release (May 12, 2025) ‘Nursing leader condemns government immigration measures in major speech.‘ ‘
‘The leader of the UK’s largest nursing union … has condemned the government’s proposed immigration measures as ‘pandering and scapegoating’. (my emphasis)
‘In her conference speech, RCN General Secretary and Chief Executive Professor Nicola Ranger said: “Many of you in this hall today started your nursing journey far away. So let me say again: you are more than welcome in the UK. Thank you for bringing your skills to this country and bringing your lives here. You know, more than I ever will, the obstacles, costs and the hostility. “But look at the Home Secretary and Prime Minister. The UK is so reliant on overseas colleagues, especially in social care. The government has no plan to grow a domestic workforce. This is about politics – pandering and scapegoating. It should be about people.
“We need an immigration system that works for care staff, nurses and the people who rely on them..”
On funding, from the Health Foundation (October 24, 2025) ‘Health Foundation responds to the Care Quality Commission’s State of Care report ‘
‘’Labour is right to talk about shifting care out of hospital and strengthening care in the community. But – a year in – our analysis shows how far the government is from having a coherent policy agenda to make these promises a reality. Detail on how change will happen is lacking and resources to deliver reform are limited. ‘
‘The CQC is right to call for investment in social care. The current social care system in England is a threadbare safety-net in desperate need of reform and investment. We estimate that meeting demand for care, covering rising costs, improving access to services, and making a meaningful and much needed improvement to care workers’ pay could cost an extra £8.7bn in 2028/29. But government funding promised for social care so far will barely be enough to meet people’s needs and cover a slight boost to pay and conditions.’’
And from the same source (October 22, 2025): ‘Social care: a year in, what prospects for reform?’
‘The £4bn extra a year in 2028/29 already announced for social care in the Spending Review was better than expected given the grim fiscal context. But much of it will come out from local council taxpayers rather than Treasury coffers.’
From the Nuffield Trust (December 18, 2025): ‘Coal or chocolate coins: What do the changes to local government funding mean for social care?’
‘We now know from the provisional Local Government Finance Settlement that up to £4.6 billion will be made available to councils for social care by 2028/29. But much of this is likely to come from increases to Council Tax rather than additional government funding. ‘
‘The Settlement also confirms that the additional government contribution to social care by 2028/29 will be the £500 million to be distributed through the social care Relative Needs Formula. This has already been promised to meet the costs of the fair pay agreement – already a tight squeeze to deliver meaningful improvements to pay and conditions. ‘The only additional new funding to be delivered by government is a share of transition funding estimated to be spent on social care, and £331 million from the NHS via the Better Care Fund. There is therefore barely enough to cover the costs of the fair pay reforms, let alone meet need and demand, or implement any recommendations the Casey commission produces.’
So the prospect of beneficial change for social care in England under a Labour government looks remote: the BBC’s ‘major factor is the crisis in social care provision’ looks as if it will remain in place with all its negative consequences for NI, Scotland and Wales!
LikeLiked by 1 person